

Minimal Residual Disease Assessment and Allogeneic Transplantation as Consolidation Therapy in Acute Lymphoblastic Leukemia
Abstract
Introduction: Detectable minimal residual disease (MRD) after therapy for acute lymphoblastic leukemia (ALL) is the strongest predictor of hematologic relapse (1-4).
Colombian reports of adults with ALL showed poor survival rates, the median OS was 12 months and the median PFS was only 7 months (5,6). Most reports from Colombia as well as Latin America did not include patients that had a transplant as an initial consolidation strategy and used MRD as prognostic factor. (7-9).
The objective of the study was to assess progression free survival (PFS) and overall survival (OS) of patients with ALL according with MRD status at end of induction therapy.
Methods: A retrospective cohort comparing PFS and OS in adults with de novo ALL, according to the MRD status at the end of induction chemotherapy, and the type of post-induction consolidation strategy used.
This research work had the endorsement of the ethics and research committees of the institutions where it was carried out.
Results: Were included 165 adults with ALL in the MRD investigational group, the basal characteristics of the population are described in table 1.There were 73 patients in the MDR negative group and 92 in the MDR positive group.
Median PFS for the MRD positive group was 11 months (CI 95% 11.7 - 22.2), and not reached for the MRD negative group (p<0.001). At three-years PFS was 18% and 55 %, respectively (p<0,001). Fig 1.
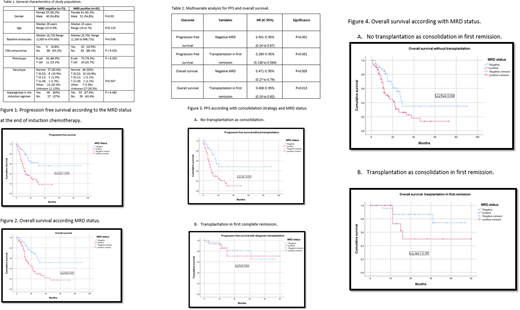
The median OS for MRD positive patients was 16 months (CI 95%, 8.8 - 23.15) and was not reached in the MRD negative group. At three-years, OS was 26 % and 51 % for the former and latter group, respectively. Fig 2.
Among subjects that were not transplanted, median PFS was 21 months for MRD negative and 9 months MRD positive patients (p<0.001). Fig 3A.
Median of PFS was not reached in either group, whereas 3-year PFS was 64% for MRD negative and 70% for MRD positive patients when transplantation in first remission was used (p=0.861). Fig 3B.
For the patients with only chemotherapy for consolidation treatment, the median OS were 16 months (IC 95% 11.32 to 20.67) for MRD positive, and 27 months IC 95% (20.91 to 33.09) in negative MRD. (p=0.004). The 3-year OS 34% for MRD negative and 22% for MRD positive patients. Fig 4A.
The individuals with allogeneic transplantation during first remission overcome de risk of death in the positive MRD status. The median OS were 16 months for positive MRD and transplantation and not reached in negative MRD group, The 3 year OS were 74% for MRD negative and 49% for MRD positive patients. (p=0.187). Fig 4B.
Multivariate analysis
At multivariate analysis, the Negative MRD status and transplantation in first remission were associated with better PFS and OS, in these patients with ALL de novo, Table 2.
Conclusion: MRD status at end of induction is an independent prognostic factor for PFS and OS in adult ALL. Allogeneic transplantation in first remission may overcome the adverse prognostic impact MRD. This is the first report that verifies the impact of MRD, on progression free survival and overall survival in the Colombian population.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal